GreyMatters
Educational articles, BetterBrain resources, latest in brain health, and news about us. Written for you, with expertise (and love).

How Chronic Stress Shrinks Your Brain, and How to Reverse It
Chronic stress does more than affect your mood. Sustained cortisol exposure physically shrinks the hippocampus, your brain's primary memory center. The encouraging part: this is reversible. In controlled neuroimaging studies, eight weeks of mindfulness practice increased gray matter in the hippocampus and reduced it in the amygdala, the brain's threat-detection center. Managing stress is one of the most accessible ways to protect your long-term cognitive health.
Stress is easy to file under "quality of life" rather than "brain health." The neuroscience tells a different story, and it's a hopeful one, because the same biology that makes chronic stress harmful also makes it one of the most modifiable risks you can act on.
Below, we cover what chronic stress does to the brain, the landmark study showing mindfulness can reverse it, the techniques that actually work, and how to measure your progress.
What does chronic stress do to your brain?
When your brain perceives a threat, it releases cortisol. In short bursts, this is helpful, it sharpens your response to a genuine challenge. The problem is sustained elevation.
Under chronic stress, prolonged cortisol exposure becomes toxic to neurons, and the hippocampus is especially vulnerable because it is packed with cortisol receptors. Over time, that exposure causes the neural branches that let brain cells communicate to shrink. The downstream effects are measurable: reduced hippocampal volume, fewer new brain cells, and impaired memory.
This matters beyond day-to-day forgetfulness. Hippocampal shrinkage is one of the earliest detectable structural changes in Alzheimer's progression, and chronic psychological stress is now recognized as a modifiable dementia risk factor in its own right. In other words, stress sits on the same biological pathway as accelerated cognitive aging, which is precisely why acting on it has such a high return.
Can mindfulness reverse stress-related brain changes?
Yes, and the evidence comes from before-and-after brain imaging, not self-report.
In 2011, researchers at Harvard-affiliated Massachusetts General Hospital published a landmark neuroimaging study. Using MRI, they measured gray matter density in healthy adults before and after eight weeks of mindfulness practice. Participants showed measurable increases in gray matter in the hippocampus and in regions involved in learning and emotional regulation. At the same time, gray matter in the amygdala, the brain's primary stress and threat-detection center, decreased. A control group who did not practice mindfulness showed none of these changes.
The design is what makes it compelling. This was not a comparison of lifelong meditators against non-meditators, where genetics or lifestyle could explain the difference. It was imaging of the same brains, across just eight weeks of practice. You can read the full study here.
How does stress management protect the brain?
Mindfulness and related practices work through a few overlapping mechanisms. They reduce cortisol output, calm the amygdala's threat response, and lower the chronic, low-grade inflammation associated with sustained stress. These are the same pathways implicated in accelerated cognitive aging, so quieting them protects the brain on more than one front at once.
The practical implication is freeing: you do not need the "perfect" technique. You need to move these levers consistently, and there is more than one way to do that.
What stress management techniques actually work?
Different techniques reach the same biology through different doors, which means you have options. These are the Essential, evidence-based interventions to start with:
- Slow, deep breathing. Controlled breathing activates your parasympathetic nervous system, your body's "rest and digest" mode. Even a few minutes measurably reduces cortisol and heart rate. For many people this is the easiest entry point.
- Mindfulness meditation. The technique behind the brain-imaging study above. Consistent practice, even 8 to 10 minutes daily, produces measurable effects on stress hormones and self-reported stress within a few weeks.
- Nature exposure. Time in natural environments is associated with lower cortisol, lower blood pressure, and improved mood. The effect appears to be dose-dependent, so more time outdoors tends to help more.
- Social support. Strong social connections help buffer the brain against the effects of stress.
How do you start a 10-minute mindfulness practice?
You do not need a cushion, an app, or a quiet mind. Here is the whole practice:
Find a quiet spot and sit comfortably. Bring your attention to the physical sensation of your breath, the air moving in and out. Your mind will wander. That is not failure, that is the exercise. Each time you notice it drifting and bring it back, you are doing the rep that builds the skill. There is no perfect posture and no requirement to empty your mind. Just ten minutes of practicing the return.
A note on getting started: Don't overthink which technique to begin with. If sitting meditation feels like a stretch, start with a few minutes of slow breathing or a walk outside. The research is clear on this point: the technique that protects your brain is the one you will actually do.
How can you track stress and its effects on the brain?
You can't feel your inflammation dropping, but you can measure it. Chronic stress shows up in bloodwork as elevated hs-CRP, one of the same inflammatory markers associated with cognitive decline. When a stress-management practice starts working, that number moves, and lab panels let you watch it happen.
The effects ripple outward from there. Sleep quality typically improves within weeks of consistent practice, and better sleep gives your glymphatic system, your brain's overnight waste-clearance crew, more time to do its job.
This is what makes stress management such a high-leverage intervention. It rarely works alone. Better stress regulation improves your sleep, better sleep amplifies the benefits of exercise, and lower inflammation makes anti-inflammatory nutrition work harder. Pull one lever, and the whole system responds.
The bottom line
Chronic stress physically changes the structure of your brain, and mindfulness and related practices can measurably change it back. You don't need to overhaul your life to benefit. Ten minutes of breathing or meditation, a walk outside, or time with people you care about all move the same biology. Start with whatever feels easiest, stay consistent, and let the results compound.
If you're working with a Brain Health Coach, the De-Stress section of your protocol is a natural starting point.
Ready to build a personalized stress management practice? Check if your insurance covers coaching.
Frequently asked questions
Does stress really shrink your brain?Yes. Sustained cortisol exposure from chronic stress is associated with reduced hippocampal volume, the brain region responsible for memory. It also reduces the formation of new brain cells and impairs memory over time.
Can you reverse brain changes caused by stress?Evidence suggests you can. In a 2011 MRI study, eight weeks of mindfulness practice increased gray matter in the hippocampus and decreased it in the amygdala in the same participants, changes not seen in a non-practicing control group.
How long does it take for mindfulness to change the brain?Structural changes were measurable after eight weeks of practice in controlled imaging studies, and effects on stress hormones and self-reported stress often appear within a few weeks.
What is the best stress management technique for brain health?There is no single best technique. Slow breathing, mindfulness meditation, nature exposure, and strong social connection all work through overlapping pathways. The most effective one is the one you will do consistently.
Is chronic stress a risk factor for dementia?Chronic psychological stress is now recognized as a modifiable dementia risk factor. Hippocampal shrinkage, which stress contributes to, is one of the earliest structural changes seen in Alzheimer's progression.
VERVE-102: A One-Time Gene Edit for Cholesterol, and Why It's a Brain Story | BetterBrain
Every so often a piece of research comes along that makes you stop and appreciate how far medicine has come. This is one of those.
Researchers just reported early results for a one-time treatment that durably lowers LDL cholesterol by editing a single gene. One infusion, with effects that have held for up to a year and a half so far, and likely to last a lifetime. It's very early research in a small, specific group of patients, and it's years from a doctor's office. But the underlying biology is some of the most well-studied in all of cardiovascular medicine, and it connects directly to your brain.
Editing one gene to lower cholesterol
The therapy, called VERVE-102, targets a gene called PCSK9. PCSK9 is a protein that reduces your liver's ability to clear LDL cholesterol from your blood. The more PCSK9 activity you have, the fewer LDL "receptors" your liver keeps available to pull LDL particles out of circulation.
Here's the reassuring part: some people are born with naturally low-functioning PCSK9 genes, and they tend to have markedly lower LDL across their entire lives, substantially lower rates of heart disease, and no apparent downside. Turning down PCSK9 is a protective pattern scientists have studied for two decades. We already have approved PCSK9-lowering drugs; they just require ongoing injections.
What's new is the delivery. VERVE-102 uses base editing, a precise form of gene editing, to make a single change to the PCSK9 gene in liver cells after one infusion, doing once, durably, what current drugs do repeatedly. In the Heart-2 trial, a single dose lowered LDL by an average of around 50%, and by as much as roughly 69% at the higher doses, with reductions holding for up to 18 months and no treatment-related serious adverse events reported.
The honest caveats
The headline is easy to over-read, so here's the careful version. It's a phase 1b trial, an early stage focused on safety and initial signals in a small number of participants, and it has not been shown to prevent heart attacks, strokes, or cognitive decline. It enrolled a specific, high-risk group (inherited very high cholesterol or early coronary artery disease), so these are not general-population results. And gene editing is genuinely new: the PCSK9 mechanism is exceptionally well understood, but a permanent edit to a gene is a young field whose long-term safety story takes years to write. The likely path is approval first for very high-risk individuals, at significant cost, after a larger phase 2 trial.
Why this is a brain-health story
At BetterBrain, we look at the whole body, because your brain doesn't exist in isolation from it, and few things connect the two as directly as lipids.
Start with ApoB. You've probably heard of LDL cholesterol; ApoB is the more precise number underneath it. Every LDL particle carries exactly one ApoB protein, so LDL-C tells you the amount of cholesterol in LDL particles, while ApoB tells you the number of particles actually driving damage in your artery walls. When the two disagree, ApoB is the better predictor of risk. Lowering PCSK9, through these new therapies or the drugs we already have, lowers both.
Now connect it to the brain. The blood vessels that feed your brain face the same lipid-driven damage as the ones feeding your heart, and that vascular damage is one of the major pathways of cognitive decline. Protecting your lipids over a lifetime is protecting your brain, especially for people who tend to run higher LDL, including APOE4 carriers. That's one reason lipid management is a core part of what we do.
What this means for you, right now
You don't have to wait for a therapy that's years away. The target itself, your lipid health, is something you can measure and move today.
Get your ApoB tested, not just standard cholesterol, because it counts the particles actually driving damage. Think of lipids as a lifelong number: it's the decades of cumulative exposure that drive risk, so small, steady improvements compound in your favor, and starting earlier beats starting perfectly. Use the levers you already have, including diet, regular movement, and, where your physician recommends them, proven medications.
If you'd like to see where you stand, BetterBrain Blueprint covers ApoB and 50+ other markers and starts at $89 with insurance, and a BetterBrain coach can pull your full lipid picture into one clear plan, so that whatever arrives in five or ten years, you've protected the decades in between.

The Glymphatic System: Why Deep Sleep Is Your Brain's Best Cleanup Tool
What if the most important thing you could do for your brain tonight was also the most straightforward? Not a new supplement or a complicated protocol. Just better sleep, specifically the deep stages most people shortchange without knowing it.
Here is the biology that makes that matter more than most people appreciate.
Your brain has its own plumbing. It only fully runs at night.
Every other tissue in your body has a lymphatic system to carry away metabolic waste. For a long time, the brain was thought to be the exception, with no obvious mechanism for the job. That changed in 2013 when researchers described the glymphatic system: a network that uses cerebrospinal fluid to flush waste out of brain tissue, including amyloid-beta and tau, the proteins that accumulate in Alzheimer's disease.
The connection to sleep came alongside it. Glymphatic clearance is not constant. It ramps up dramatically during deep, slow-wave sleep, when the spaces between brain cells expand and fluid can move through more freely. This is one of the clearest biological explanations for why sleep is not optional maintenance. It is when a specific, measurable cleanup process actually runs, protecting your brain now and building resilience for decades to come.
What the newer research tells us about the engine
The system's existence has been well established for over a decade. What researchers kept working on was the mechanics: what physically moves the fluid?
A 2025 study published in Cell from Maiken Nedergaard's lab (one of the teams behind the original glymphatic work) helps answer that. In mice, the team found that during deep sleep a small brainstem region called the locus coeruleus releases norepinephrine in slow, rhythmic waves, roughly one every fifty seconds. Each wave gently tightens and relaxes the blood vessels, and that slow oscillation appears to drive cerebrospinal fluid through the brain, moving waste along.
The result connects three things already known to be related (deep sleep, blood-vessel tone, and fluid clearance) into a single mechanism. Deep sleep is not the brain idling. It is the brain running a coordinated pump.
Two points of context worth holding on to. First, this is animal research. The mechanism has been demonstrated in mice, whose sleep biology is a strong but imperfect model for humans. It tells us how the system likely works, not the conclusion of a human clinical trial.
Second, the same study found that zolpidem (the active ingredient in Ambien) suppressed these norepinephrine waves in mice and reduced fluid flow. That is a genuinely interesting signal, but it is a finding in animals about a mechanism, not evidence that a prescription harms people. If you take a sleep aid, this is not a reason to stop. It is a reason to make sleep quality a real conversation with your prescriber.
What this means in practice
None of this requires a new gadget. It gives you a sharper reason to take the fundamentals seriously.
Protect the deep-sleep window. Slow-wave sleep is concentrated in the first half of the night. A consistent wake time, morning light exposure within thirty minutes of getting up, and a cool, dark room are the most reliable ways to support it. These are habits that compound over years.
Be honest about alcohol and late meals. Both fragment the deep-sleep stages where clearance is most active. You may fall asleep quickly and still miss the part of the night that matters most for this system.
Treat sleep as something measurable. The same way we use biomarkers to track what is working, sleep consistency and quality are worth paying attention to over time rather than estimating from how you feel in the morning.
Take loud snoring or daytime exhaustion seriously. Both can signal sleep apnea, which repeatedly disrupts the deep sleep this system depends on. It is common, often undiagnosed, and very treatable.
If you use a sleep medication, bring the goal of better sleep quality to your prescriber rather than changing anything on your own.
BetterBrain's brain health coaches work with clients to turn sleep from a vague intention into a specific, trackable practice built around your schedule, your biology, and your data. Think sharper now, and protect your brain for decades.

Tommy Wood's 3-S Model: The Science Behind Future-Proofing Your Brain
The Framework Behind What We Do at BetterBrain
Our Chief Science Officer Tommy Wood published The Stimulated Mind in March 2026, and we think it's the most complete, accessible guide to dementia prevention that exists right now. A rigorous, science-backed model for understanding what your brain actually needs across a lifetime, written by someone who has spent his career studying exactly this.
At the center of the book is what Tommy calls the 3-S Model: Stimulation, Support (sleep and recovery), and Supply (of energy and nutrients). These aren't three separate suggestions. They're three categories of input the brain depends on, and Tommy's argument is that they reinforce each other in ways most people don't appreciate. They synergize, providing outsized benefits from even simple changes across all three.
BetterBrain is built around exactly this model. The 10 health systems and 11 practices our coaches work through with you are the operational version of what Tommy lays out in the book. Here's a breakdown of each S and one thing you can act on this week.
S1: Stimulation
The first S is the one that surprises people. Tommy's argument is that the brain, like muscle, needs ongoing challenges to maintain its structure. The variable that matters is novelty. Doing the same crossword every day is not stimulation in the sense your brain cares about. Learning a language, picking up a new instrument, or taking a class on something you have no prior context for, are stimulating.
This connects to what researchers call cognitive reserve: the buffer your brain builds through years of varied learning. Cognitive reserve is one of the strongest predictors of who maintains function in their 70s and 80s, even in the presence of pathology like amyloid plaques.
What you can do this week: Pick one thing this month that you don't already know how to do. It doesn't have to be heavy, a new recipe technique, a new fitness class, a new route on your morning walk that requires you to navigate. The brain treats novelty as a signal that it needs to keep adapting.
S2: Support (Sleep and Recovery)
The second S is the one most people know is important and still underestimate. Recovery, especially during sleep, is when the brain adapts and improves.
While you sleep, your brain runs a waste-clearance system that flushes out the proteins that build up during the day, including amyloid, the same protein that accumulates in Alzheimer's disease. Think of it like a dishwasher that only runs at night. Skip enough nights, or get consistently shallow sleep, and the dishes pile up. Disrupted sleep is associated with elevated pTau-217, lower cognitive scores, and higher long-term dementia risk.
Tommy is direct about this in the book: there is no supplement protocol that compensates for chronically poor sleep. And the work has to start with the structure of your sleep itself, meaning how much time you actually spend in the deep and REM stages, not just how many hours you're in bed. You can sleep eight hours and still miss most of the stages where the real restoration happens.
What you can do this week: Protect a consistent wake time. The wake time matters more than the bedtime because it anchors your body's internal clock. Pair it with morning light within 30 minutes of getting up, and you've done more for your sleep quality than most people manage with supplements or sleep trackers alone.
S3: Supply (Energy and Nutrients)
The third S is where a meaningful part of your biomarker picture lives. Your brain runs on a continuous supply of glucose, oxygen, omega-3 fatty acids, B vitamins, and a long list of micronutrients. Deficits in any of these can quietly compromise function for years before they show up as symptoms. When these markers are at optimal levels, they actively protect your brain, often for decades.
The first place to look is diet. What you eat every day is the primary driver of whether your brain gets what it needs. Targeted supplementation comes second, once you know where the gaps actually are.
The biomarkers we look at first in the Blueprint panel are homocysteine, vitamin D, vitamin B12, ferritin, and folate. These are the ones most likely to flag a nutrient supply problem before you feel it. And the fix is usually targeted, not maximal. Most clients don't need fifteen supplements, they need the right two or three, chosen based on what their labs actually show.
What you can do this week: If you haven't had a full brain-health panel in the past year, that's where to start. A nutrient gap rarely shows up in isolation, and the right intervention depends on seeing how everything fits together.
Why All Three Matter Together
The argument the book makes is that the components that support brain health aren't a long list of individual variables, they're an integrated network.
Stimulation without sleep doesn't give the brain time to consolidate. Sleep without nutrient supply leaves the brain trying to do its overnight work without raw materials. Nutrient supply without stimulation gives the brain everything it needs to grow but no reason to.
This is consistent with what BetterBrain's coaches see in practice. Clients who work hard on one of the three but ignore the others tend to plateau. The ones who address all three see the biggest shifts in biomarkers, cognitive scores, and how they actually feel.
The Bottom Line
The Stimulated Mind is the best communication of modern brain science available today, worth reading whether you're at the beginning of thinking about brain health or several years into a protocol.
Working with a BetterBrain coach to address all three Ss, across all 11 practices, is how you turn a framework into measurable results.
hs-CRP: The Biomarker Most Likely to Flag Silent Inflammation in Brain Health
If you have ever had a routine blood panel, you have probably seen "CRP" on the list. What you may not have seen is "hs-CRP," which sounds like the same test but is not. The difference matters a lot for brain health.
This piece walks through what hs-CRP measures, why it shows up in almost every BetterBrain protocol, and what to do if yours is elevated.
What hs-CRP measures
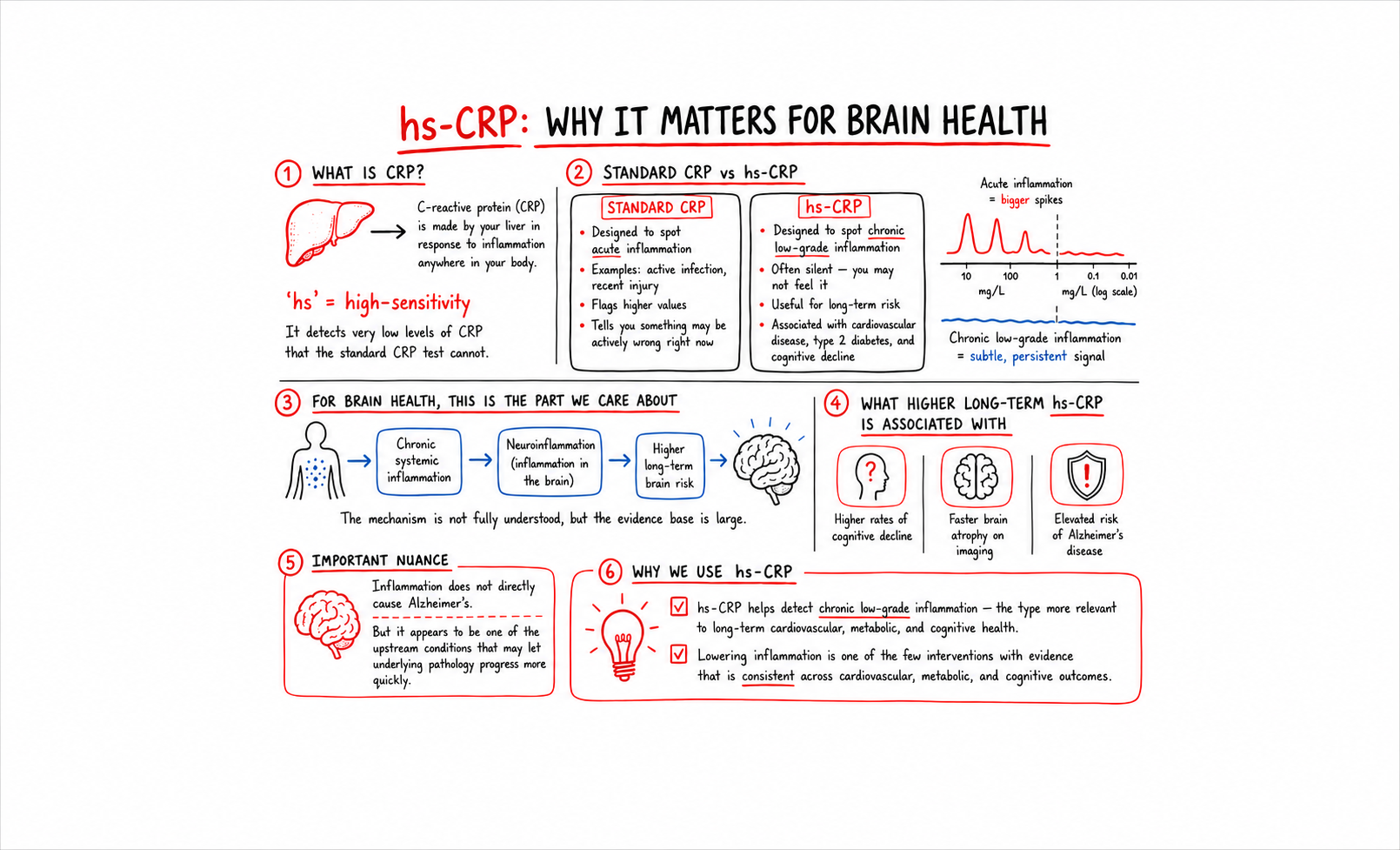
C-reactive protein is made by your liver in response to inflammation anywhere in your body. The "hs" stands for "high-sensitivity," which means the test can detect very low levels of CRP that the standard CRP test cannot.
This distinction sounds technical but it is the whole reason we use hs-CRP and not standard CRP. Standard CRP is designed to spot acute inflammation, like an active infection or a recent injury. The values it flags are high enough to indicate something is actively wrong right now. hs-CRP is designed to spot chronic low-grade inflammation, the kind that does not feel like anything but is associated with long-term risk for cardiovascular disease, type 2 diabetes, and cognitive decline.
For brain health, the chronic low-grade version is the one that matters.
Why this matters for your brain
Chronic systemic inflammation is associated with neuroinflammation, the inflammatory state of the brain itself. The mechanism is not fully understood, but the body of evidence is large. People with higher long-term hs-CRP have higher rates of cognitive decline, faster brain atrophy on imaging, and elevated risk of Alzheimer's disease.
Inflammation does not directly cause Alzheimer's. But it appears to be one of the upstream conditions that lets the underlying pathology progress more quickly. Lowering it is one of the few interventions where the evidence is consistent across cardiovascular, metabolic, and cognitive outcomes.
What the numbers mean
- Optimal: under 1.0 mg/L
- Borderline: 1.0 to 3.0 mg/L
- High: above 3.0 mg/L
Most standard labs flag a result only when it crosses 3.0 mg/L or higher. The 1.0 to 3.0 range is where a meaningful number of clients are quietly running elevated. Their primary care has waved it off as "in range." For brain health purposes, it is not.
The biomarkers that pair with hs-CRP
A single hs-CRP value is informative but more useful in context. The markers to look at alongside it:
Homocysteine. Elevated homocysteine is associated with both inflammation and methylation problems. If hs-CRP and homocysteine are both elevated, the inflammation is likely driven in part by nutrient gaps.
ApoB and Lp(a). Cardiovascular markers. Elevated hs-CRP plus elevated ApoB is a particularly bad combination for vascular brain health.
HbA1c and Fasting Insulin. Metabolic markers. Glycemic dysfunction drives systemic inflammation. If hs-CRP is elevated, look here next.
Ferritin. Iron storage. Elevated ferritin can indicate underlying inflammation, separate from iron status.
The picture you assemble from these markers tells you whether the inflammation is metabolic, vascular, nutrient-driven, or something else.
What to do about it
The interventions that consistently move hs-CRP overlap with the interventions that consistently move long-term cognitive trajectory. Sleep, glycemic control, omega-3 status, dental health, gut health, and visceral fat reduction are all associated with lower chronic inflammation over time. None of them are quick fixes. All of them compound.
For BetterBrain clients with elevated hs-CRP, the coaching protocol usually starts with the highest-leverage area their panel reveals. A client whose hs-CRP is elevated alongside high HbA1c starts with glycemic control. A client whose hs-CRP is elevated alongside high homocysteine starts with methylated B-complex and a closer look at folate, B12, and B6 intake. The technique is to follow the panel.
Find out where you stand
hs-CRP is one of the most useful brain-health markers in routine bloodwork, and one of the most commonly missed. If you have not had a high-sensitivity version of CRP measured in the past year, it is worth checking.
BetterBrain Blueprint covers hs-CRP alongside 50+ other markers and starts at $89 with insurance.
.png)
The Essential Techniques our coaches keep recommending for brain health
We use the term Essential Techniques inside BetterBrain a lot. Each BetterBrain Practice (Move, Sleep, Eat, De-Stress, and so on) is made up of specific techniques, and the Essential Techniques are the ones our panel of clinical advisors identified as the techniques with the greatest evidence and broadest applicability.
These are not techniques for a specific kind of client. They are the techniques worth considering for almost everyone thinking about long-term brain health, regardless of starting point, age, or risk profile. About 15 to 20 percent of the techniques in our library are Essential. The other 80 to 85 percent are context-dependent, applied when a client's panel or situation calls for them. A coach builds a personalized action plan by looking across the whole library, deciding which Essentials to elevate first and which context-dependent techniques to layer in. The Essentials are the foundation underneath every plan.
We asked some of our coaches what trends they are seeing across the clients they work with, and which Essential Techniques those trends keep pointing back to.
The post-meal walk (Move Practice)
Maggie works with clients across the metabolic-health side of our client base. The trend she keeps seeing: HbA1c and fasting insulin numbers creeping into pre-diabetic ranges, often without the client realizing it. Many of them are exercising, but most of them are not walking after meals.
"Ten minutes after each meal. That is the rule I get the highest compliance on, because nobody can argue they don't have ten minutes. And it does more than people expect."
This is one of the Essential Techniques in our Move Practice because the evidence is broad and the bar to entry is low. A short walk after eating blunts the post-meal glucose spike. Repeated over months, it is one of the most reliable ways we have seen to shift HbA1c, fasting insulin, and the metabolic conditions that drive midlife brain atrophy. The cost is nothing, the schedule disruption is minimal, and the long-term payoff compounds. It is essential because it works for almost everyone.
Consistent wake time and morning light (Sleep Practice)
Emily works with a large share of our clients who came to BetterBrain because of family history of dementia. The trend she keeps seeing: anxious clients arriving with long supplement lists, wanting to talk about pTau-217 and APOE4, while sleeping six or fewer hours a night.
"One night of four hours isn't really the question. The question is why someone is typically sleeping four or five hours at most. Patterns matter. What we identify from the first visit and where we end up is more than one night of poor sleep. Sleep is the foundation. Exercise goals, stress management, eating, they all land once sleep patterns are optimized."
The Essential Technique Emily points to first is in our Sleep Practice: a consistent wake time paired with morning light. The reason this is essential for almost everyone is the glymphatic system. Sleep is the period during which the brain runs its only clearance system, including the clearance of amyloid. A consistent wake time anchors the circadian rhythm, and morning light reinforces it. The evidence is strong, the intervention is free, and it works for clients in their 30s and their 70s.
Strength training (Move Practice)
Wendy works with many of our clients in their late fifties and sixties. The trend she keeps seeing: clients who are doing aerobic exercise faithfully, often three or four days a week, and skipping strength training entirely.
"I'm flexible with many aspects of a health plan, but strength training is one area I strongly encourage people not to overlook. The research connecting muscle mass and brain health after 50 is incredibly compelling, and maintaining strength now can have a major impact on long-term health and quality of life."
Strength training is another Essential Technique in our Move Practice. The reason it is essential, not optional: muscle is the primary site of glucose disposal in the body, the pathways linked to neurogenesis are responsive to resistance training, and sarcopenia is one of the strongest predictors of cognitive decline in older adults. The evidence supports two sessions a week, moderate intensity, sustained for at least six months. Bodyweight work and resistance bands are enough to start. The technique is essential because everyone past 30 is slowly losing muscle, and the cost of skipping it is too high.
Methylated B-complex (Supplement Practice)
Another trend we keep seeing across our client base: people arriving with homocysteine in the 11 to 14 range, told by their primary care that it is fine. The gap between what is flagged at most labs and what is optimal for brain health is one of the cleanest examples of where our framework differs from standard care.
The optimal range for homocysteine is under 9 μmol/L. Most labs flag a result only above 15. The 9 to 14 range is where a meaningful number of clients are quietly carrying elevated risk that has been waved off. A methylated B-complex moves the marker for the majority of clients within three months, and the cognitive payoff is real.
The Essential Technique in our Eat Practice is targeted methylated B-complex supplementation. The reason this is essential for almost everyone has to do with the underlying biology. Homocysteine is cleared through methylation pathways that depend on the active forms of folate, B12, and B6. A significant portion of the population carries variants of the MTHFR gene that reduce how well the body converts standard folic acid into the active form. Methylated B-complexes deliver the active forms directly. For anyone over 40 thinking about long-term brain health, this is one of the highest-leverage interventions available.
What the pattern reveals
Across our coaches with different specialties and different client populations, the same Essential Techniques keep coming up. These are the techniques that consistently move the needle, regardless of who is doing them. What our coaches actually do day to day is build action plans that span the full technique library, prioritizing among the Essentials and layering in the context-dependent techniques that fit each client's panel and life.
The Essentials are universal. The action plan is personal.
Find out where to start
If you'd like a quick read on which Essential Techniques to prioritize based on what you are already doing, take the free Essential Scan. Open to anyone, whether you're already a BetterBrain client or just starting.
If you'd like a deeper personalized action plan, BetterBrain coaching pairs you with a Brain Health Coach who builds the plan with you. Coaching is covered at $0 for 92% of approved clients with qualifying insurance.
Get immediate insights with a 3 minute assessment
Start now.png)
GreyMatters
Saunas and Alzheimer's: Hot Topic or Just Hot Air?
For centuries, saunas have been lauded for their supposed health benefits, from improved cardiovascular function to detoxification. The recent trends around longevity seem to have revitalized the use of saunas, now considered a popular "health hack". But could spending time in these heated chambers also benefit your brain? Recent research suggests that sauna use might indeed play a role in mitigating the risk of Alzheimer's disease. In this article, we'll explore the scientific evidence behind this claim and consider how sauna use may impact your brain health.
The Connection Between Saunas and Alzheimer's Disease
The Finnish Study
A study from Finland has brought attention to the potential benefits of saunas for brain health. According to the 2,315 person study1, men who used a sauna 4-7 times a week showed a 65% reduced risk of Alzheimer's disease compared to those who used it once a week. Although the study mainly focused on men and thus requires further exploration for generalization, the findings are promising - 65% is a staggering number. If true, this would imply we could cut Alzheimer's prevalence from 6 million to 2 million in the US if only everyone used the sauna daily!
The Underlying Mechanisms
Scientists have proposed several mechanisms through which saunas may benefit the brain. One suggestion is that saunas can significantly improve sleep quality and time in deep sleep, which improves the brain's ability to clear toxic proteins. Moreover, heat stress activates heat shock proteins that can repair damaged proteins, which may play a role in neurodegenerative diseases like Alzheimer's. Lastly, saunas may improve various markers of vascular function, such as blood pressure and blood circulation, known risk factors for Alzheimer's.
Caveats and Considerations
First, the impact was more muted for those who used the sauna only 2-3 times a week (~22% risk reduction). Additionally, while the Finnish study shows a correlation, and certainly attempted to control for relevant variables, it is always very challenging to prove causation in retrospective studies.
Conclusion
The notion that saunas could "incinerate" your Alzheimer's risk is captivating, they should not be viewed as a standalone solution. While promising studies hint at a beneficial correlation, saunas are not a guaranteed prevention method for Alzheimer's. However, given their other health benefits and the intriguing data suggesting a potential role in brain health, saunas could be a worthwhile addition to your wellness routine. Plus, who doesn't enjoy an intense sauna session followed by a cold plunge or shower?
Why Is Alzheimer's More Common in Women?
When it comes to Alzheimer's disease, gender plays an undeniable role. A staggering two-thirds of those diagnosed with Alzheimer's in the United States are women. This disparity has puzzled researchers for years. Initially, many attributed it to the longer lifespan of women compared to men. However, as our understanding of the disease deepens, we've learned that longevity alone doesn't fully explain the 2X difference in prevalence.
The Longevity Theory Falls Short
For a long time, the prevailing explanation for why more women than men were diagnosed with Alzheimer's was simple: women live longer, and Alzheimer's is a disease that primarily affects older adults. However, this explanation has increasingly come under scrutiny. As it turns out, the difference in lifespan between men and women isn't sufficient to account for the wide gap in Alzheimer's cases. The narrative is much more nuanced and involves a complex interplay of biological and social factors.
The Menopause Transition Hypothesis
Menopause is a significant biological milestone in a woman's life, marked by the end of menstrual cycles and fertile years. One of the most significant changes that accompany menopause is a decline in estrogen levels. Estrogen is not just a reproductive hormone; it also has protective effects on the brain. The sharp decrease in estrogen during the menopause transition has been hypothesized to elevate the risk of Alzheimer's among women. In fact, cognitive decline associated with reduced estrogen levels has been reported, especially during the peri-menopausal and post-menopausal phases.
A beacon of hope: Hormone Replacement Therapy (HRT)
Given the hypothesized link between menopause and Alzheimer's risk, Hormone Replacement Therapy (HRT) has been studied as a potential preventive measure. Some evidence indicates that HRT could mitigate the risk of Alzheimer's among post-menopausal women. One prospective study1in particular demonstrated a 41% reduction in the risk of Alzheimer's in women who did HRT vs those who did not. Of course, any decision to start HRT should be made through a physician who can account for all contraindications.
The Often Overlooked Role of Caregiving
The gender disparity in Alzheimer's doesn't end with disease prevalence; it also manifests in caregiving. Women make up a significant majority of Alzheimer's caregivers, often bearing the emotional and physical burden of caring for afflicted family members. This role can lead to heightened stress levels, which in turn could potentially impact a woman’s own cognitive health.
Conclusion
The question of why Alzheimer's disproportionately affects women is far from straightforward. While the longevity theory has been partially debunked, the menopause transition and its hormonal changes offer a compelling avenue for understanding the gender disparity in Alzheimer's prevalence. Even social factors like caregiving roles cannot be discounted. Understanding these contributing factors can pave the way for gender-specific preventive strategies, which are beginning to be implemented in clinical practice.
Should you get tested for APOE4?
Chance are, you know someone who has tested for their APOE genotype. With the advent of consumer genotyping companies such as 23andme, genetic testing for Alzheimer's risk has become increasingly accessible, with the APOE4 gene variant taking center stage in the discussion. The question that many people are asking is: Should I get tested for APOE4? This article aims to provide a balanced perspective, detailing the pros and cons to help you make an informed decision.
What Is APOE4?
The APOE gene produces a protein essential for fat metabolism and is involved in brain cell repair. There are three main variants of this gene—APOE2, APOE3, and APOE4—with the APOE4 variant being strongly associated with an increased risk of developing Alzheimer's disease. While having this gene variant doesn't guarantee that you'll develop Alzheimer's, it can significantly elevate your risk. 20-25% of people have 1 copy of APOE4, conferring a 2-3X increase in Alzheimer's risk, while 2-3% of people have 2 copies, which implies an 8-10X increase in risk.
Advantages of APOE4 Testing
Empowers You to Make Informed Choices
Perhaps the most compelling reason for getting tested is the ability to make informed decisions about your health. There are specific recommendations for those carrying APOE4 such as significantly increasing DHA consumption given impaired absorption. Additionally, research suggests that APOE4 carriers get even more benefit from a range of interventions than non-carriers. In fact, some experts suggest that by applying the right interventions, you can completely mitigate the impact of having a copy of APOE4.
Opens opportunities for clinical trials and futures therapies
There is a significant research focus on APOE4 and potential pharmacological approaches to mitigating the associated risk. Testing may open up avenues for participating in such trials. Furthermore, as therapies get approved in the future for APOE4 carriers, you'll be well positioned to take advantage.
Offers Information for Family Planning
Your genetic makeup doesn't just affect you; it could also be informative for your family members. Given the heritability of the gene, knowing that you carry the APOE4 variant could give valuable insights into your relatives such as parents who may be at higher risk for developing dementia.
Drawbacks of APOE4 Testing
Carries Emotional and Psychological Weight
Although APOE4 is simply a risk factor and is far from being deterministic, finding out that you're at higher risk for Alzheimer's can be emotionally taxing. While the REVEAL study1 showed that disclosing ApoE4 status did not cause clinically significant anxiety or depression after 6 month follow up, responses are of course very individualized. Before taking the test, consider whether you're emotionally prepared for the results.
Doesn't Guarantee Prevention or Cure
At present, there is no cure for Alzheimer's. Knowing you have the APOE4 gene can offer a sense of urgency to adopt preventive measures, but it doesn't guarantee that you'll be able to ward off the disease.
Raises Ethical and Privacy Concerns
Genetic testing often brings up privacy issues. There's always the risk of data leaks or misuse by third parties, including insurance companies, even though laws exist to prevent genetic discrimination (e.g., GINA for health insurance). Be aware of these concerns when contemplating testing.
The Decision is Yours to Make
Choosing whether to undergo APOE4 testing is a deeply personal decision that should be based on multiple factors, including your emotional readiness, family history, and the current state of your cognitive health. Regardless of your decision, remember that the genetics are just one piece of a very complicated puzzle.